Myofunctional Therapy for Sleep Apnea: Where It Fits
Orofacial myofunctional therapy is often either oversold as a "miracle cure" or dismissed too quickly as "nonsense." The truth is somewhere in the middle. Think of it as physical therapy for your airway behavior—it’s not a replacement for medical treatment, but it can be a powerful tool for the right patient.
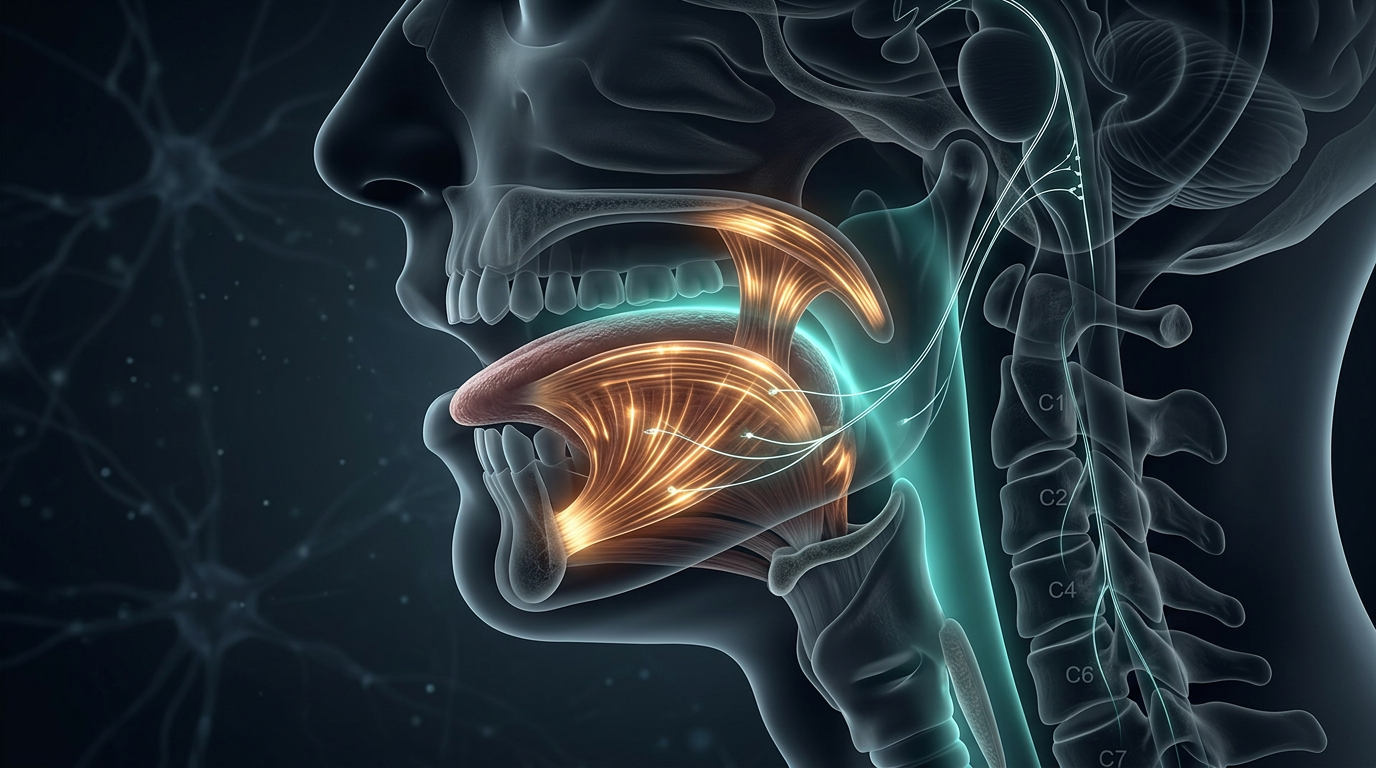
Just like you can go to physical therapy to strengthen your knee or shoulder, Myofunctional Therapy involves exercises to strengthen the muscles in your tongue, mouth, and throat.
The goal is to improve your "tongue posture" and keep your airway from being as "floppy" during sleep. It can be helpful for:
- Reducing loud snoring.
- Helping with mild cases of sleep apnea.
- Helping people who have a habit of mouth breathing.
It takes time and daily practice (like any exercise routine), and it works best as an *addition* to other treatments, not as a replacement for things like CPAP in serious cases.
Orofacial Myofunctional Therapy (OMT) consists of isotonic and isometric exercises targeting the oral and oropharyngeal structures (tongue, soft palate, and lateral pharyngeal wall).
Physiological Rationale
The stability of the upper airway is determined by both anatomy and muscle tone. OMT aims to increase the tone of the airway dilator muscles (like the genioglossus) and improve tongue positioning to reduce the "collapsibility" of the airway during sleep.Clinical Evidence
Meta-analyses have shown that OMT can reduce the Apnea-Hypopnea Index (AHI) by approximately 50% in adults with mild to moderate OSA and can improve oxygen saturation and snoring intensity.- As Adjunctive Therapy: OMT is particularly useful for patients who have "residual" snoring or mild apnea despite other treatments, or for those transitioning from mouth to nasal breathing.
- Pediatric Context: In children, OMT can be a vital part of "post-surgical" care after tonsillectomy to prevent the persistence of mouth-breathing habits.